South Africa has a tobacco control problem.
Not because we don't know smoking is harmful.
Not because we haven't increased taxes.
Not because we haven't produced regulations.
Not because we haven't issued warnings.
No, South Africa's tobacco control problem is much simpler.
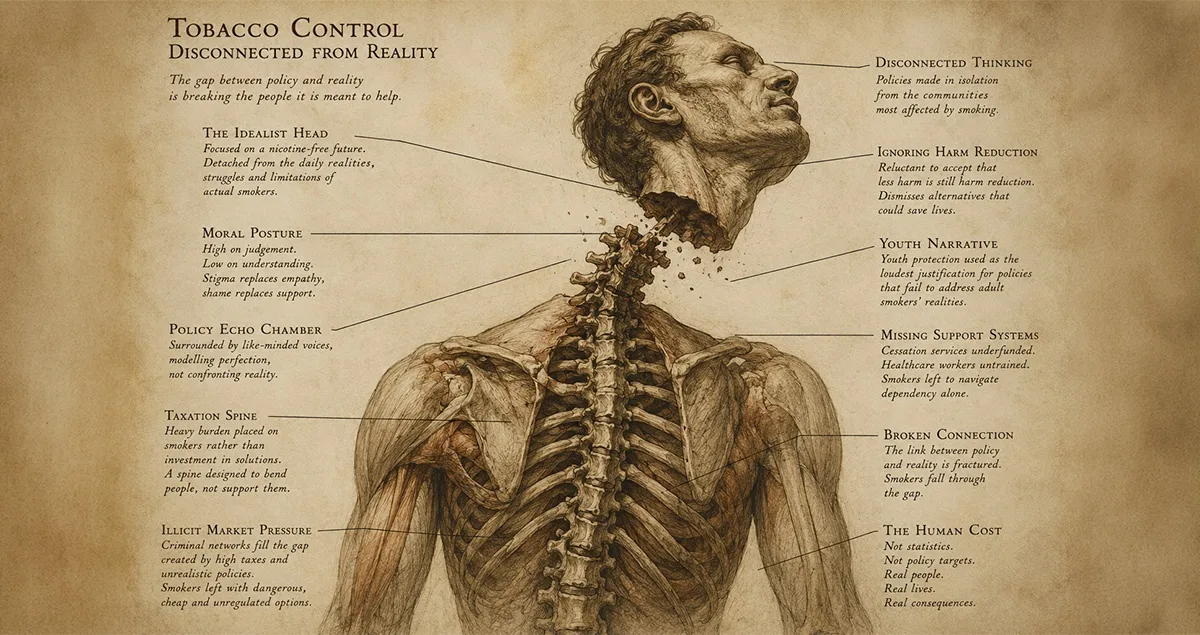
It has become detached from reality and the people it claims to help.
Somewhere along the way, tobacco control stopped being about smokers and started being about everyone except smokers. The conversation today is dominated by youth, non-smokers, future generations, nicotine-free societies and aspirational endgames.
Meanwhile, the millions of South Africans who actually smoke have become little more than supporting characters in a story supposedly written about them.
And they are paying the price.
The Smoker Who Doesn't Exist
Listen carefully to modern tobacco control discussions, and you will notice something curious.
We hear about preventing future smokers nicotine users.
We hear about protecting young people.
We hear about denormalising tobacco nicotine use.
We hear about creating a smoke-free nicotine-free generation.
The smoker is almost always absent.
Notice the shift?
But what about the people smoking today?
What about the person who has smoked for twenty, thirty or forty years?
The person who has tried to quit five, ten, or fifteen times?
The person who started smoking at fourteen and is now fifty-five?
The person who desperately wants to stop but hasn't found a way that works?
In a strange twist of public health logic, the people at greatest risk of smoking-related disease have become the least visible participants in the debate.
Taxing Addiction While Calling It Healthcare
Public health authorities often defend tobacco taxation on the grounds that higher prices reduce smoking.
In principle, they are right.
But principles have a habit of becoming awkward when they collide with reality. Most smokers did not wake up at thirty-five and decide to become nicotine dependent.
Most started as teenagers.
Many became addicted before they left school and didn't fully understand the consequences.
Yet today they are told that the solution to their dependency is to simply quit or pay more.
Imagine if we approached any other chronic dependency this way.
"We recognise you have a dependency."
"We understand you struggle to stop."
"We know repeated failure is common."
"Our solution is to make it progressively more expensive."
That would sound absurd.
Yet this is presented as enlightened public health policy.
Taxation may have a role to play.
But taxation without meaningful support increasingly looks less like healthcare and more like punishment.
The Curious Case Of The Missing Cessation Strategy
If taxation is designed to encourage quitting, one might reasonably ask:
Where is the national quitting strategy?
The National Department of Health's planning documents contain extensive detail on major health priorities, targets and programmes. Yet smoking cessation remains remarkably difficult to find as a visible, standalone national priority.
Research among healthcare professionals in Soweto found that more than 80% were willing to provide smoking cessation support. Only about one-third had ever received training to do so.
Think about that for a moment.
The people on the front lines are willing to help. But the system is not adequately equipping them.
South Africa appears to have a tobacco control strategy. What is less clear is whether it has a smoking cessation strategy.
Those are not the same thing.
The Illicit Market That Disrupts It All
The standard economic model is elegant.
Increase cigarette prices.
Smoking becomes less affordable.
People quit.
Unfortunately, South Africa insists on being South Africa.
Reality has introduced a complication.
The illicit cigarette market, which now accounts for between 70 and 75 per cent of all cigarettes sold.
For many South Africans, the choice is no longer between smoking and quitting.
It is between a legal cigarette, an illicit cigarette and an alternative product that may cost ten times more upfront.
When a packet of illicit cigarettes can be purchased for around R10, a fully taxed packet is up to five times that price, while a disposable vape costs around R100, public health messaging suddenly finds itself competing with mathematics.
And mathematics tends to win.
A smoker facing economic hardship, who happens to be the majority in South Africa, does not perform a long-term risk-benefit analysis.
They ask a much simpler question:
"What can I afford today?"
The answer is often not the one policymakers hoped for.
The Harm Reduction Heresy
Perhaps nowhere is the disconnect more obvious than in the treatment of harm reduction.
Consider two smokers.
The first switches completely to nicotine gum.
The second switches completely to vaping.
Both stop smoking.
Both eliminate combustion.
Both continue using nicotine.
One is often viewed as a public health success.
The other remains a subject of endless controversy and, in some circles, is deemed a bigger problem than combustible tobacco.
Which raises an uncomfortable question.
What exactly is the problem we are trying to solve?
Smoking?
Or nicotine?
Because those are very different things.
If nicotine itself is the enemy, then nicotine gum should be treated with the same suspicion. If smoking-related disease is the enemy, then eliminating combustion should be celebrated regardless of how it is achieved.
Yet modern tobacco control increasingly appears uncertain about which objective it is pursuing. Or maybe the objective has changed.
When Tobacco Control Became Nicotine Control
Historically, tobacco control focused on smoke.
The concern was cancer.
Heart disease.
Emphysema.
Stroke.
The devastation caused by inhaling the products of combustion.
Today, however, much of the debate has shifted towards nicotine itself.
And that shift deserves scrutiny.
Nicotine replacement therapies remain widely available and approved. They are accepted because they deliver nicotine without smoke. That principle seems straightforward.
Until someone delivers nicotine without smoke through a product that did not originate from the pharmaceutical industry.
Suddenly, the conversation changes.
The question no longer appears to be whether smoking has stopped. The question increasingly becomes who is providing the nicotine.
That is a discussion worth having honestly.
The HIV Lesson We Have Forgotten
South Africa has invested enormous resources into HIV prevention, treatment and support.
And rightly so.
Public health officials recognised long ago that simply telling people to abstain was not enough.
Reality mattered.
Human behaviour mattered.
People's circumstances mattered.
So South Africa built systems around those realities. Condoms are distributed. PrEP (Pre-Exposure Prophylaxis) is available. Testing is promoted. Treatment is provided. Counselling is offered.
The philosophy is simple.
Public health succeeds when it engages with reality rather than pretending reality will eventually surrender.
No one suggests that condom distribution encourages risky behaviour. No one argues that PrEP should be banned because abstinence is theoretically possible. No one believes treatment should be withheld until perfect behaviour is achieved.
Why?
Because public health has learned an important lesson. People do not always behave ideally. The solution is not to abandon them. The solution is to reduce harm while continuing to encourage better outcomes.
Yet when smoking is involved, this principle suddenly becomes controversial.
The Youth Argument
Whenever these questions are raised, the discussion quickly returns to youth.
And protecting young people is important.
Few would disagree.
But if youth protection is truly the primary concern, where is the enforcement?
South Africa already prohibits sales and/or supply of tobacco products to minors. Age restrictions already exist for these products and need to be extended to all nicotine products.
Yet underage access and consumption remain a reality. In 2021, the South African Global Adult Tobacco Survey highlighted that nearly a quarter of young South Africans between the ages of 15 and 24 used cigarettes.
This raises another uncomfortable question.
Why does so much attention focus on creating new restrictions while comparatively little attention appears focused on enforcing existing ones?
Protecting young people is essential.
Using young people as the sole justification for policies that affect 11 million adults is a different matter entirely.
A public health strategy should be capable of doing both.
Protecting youth and helping adult smokers are not mutually exclusive goals.
The Reality Gap
The tragedy of South African tobacco control is not that we have failed to recognise the dangers of smoking.
The tragedy is not that South Africa has failed to recognise the harms of smoking.
The tragedy is that we have become so focused on the destination that we have stopped paying attention to the people trying to get there.
For decades, public health has evolved beyond the idea that simply telling people to change their behaviour is enough.
We understand that people need support to lose weight.
We understand that people need support to manage harmful dependencies.
We understand that people living with HIV need support and strategies to prevent further infections.
We understand that people need support to adhere to treatment.
In every one of these areas, public health has learned the same lesson:
Good intentions do not change behaviour. Practical solutions and support do.
Yet when it comes to smoking, South Africa's approach often feels remarkably different. We have built an extensive framework designed to discourage smoking. What we have not built is an equally visible framework designed to help smokers stop.
The result is a policy environment that seems far more comfortable talking about smokers nicotine users' than talking to them.
Far more comfortable taxing them than supporting them.
Far more comfortable pursuing ideal outcomes than confronting imperfect realities.
And it is in that gap between aspiration and reality that millions of South African smokers continue to live.
Not as statistics.
Not as policy targets.
But as people.
Yet when the subject is smoking, many regard this approach as entirely reasonable.
The result is a policy environment increasingly disconnected from reality.
One where illicit cigarettes flourish.
Where cessation services remain non-existent in communities that need them most.
Where healthcare workers want to help but lack training and funding.
Where safer alternatives remain inaccessible to many of the people who could benefit most.
And where the people at greatest risk of smoking-related disease are often treated as though they are the least deserving of compassion.
The uncomfortable truth is that South Africa does not have a smoking problem.
It has a reality problem.
And until tobacco control begins engaging honestly with the realities faced by smokers and nicotine users, the people who will continue paying the price are the very people the system claims it wants to help.
But then again, maybe it is just a claim.